
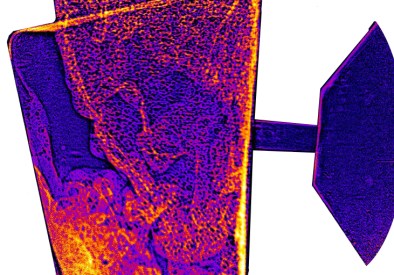
Left: propellant cylinder (CC). Right: X-ray image of propellant inside inhaler (© 2018 D. Duke)
Following recent media coverage of our research into the reduction of greenhouse gases in metered-dose inhalers (such as asthma puffers), a number of common questions have arisen about this work. Below, I answer some of those questions, and will add citations to published research as time permits.
- What is the underlying science?
At a fundamental level, we are studying the fluid mechanics of metered-dose inhalers such as asthma puffers. These devices work by releasing a small quantity of propellant (a liquid which boils to a gas at room temperature and pressure). The drug is either suspended as small particles in the propellant, or dissolved in it, along with a few other chemicals required to improve the solubility and shelf life. When the propellant leaves a small nozzle in the inhaler, it does so at high speed, forming a spray, which fragments the liquid into an aerosol which you can then breathe in. The fluid flow inside an inhaler is very complex, as it is a mixture of gas, liquid and solid particles, is boiling as it flows, and can also be turbulent. Predicting the flow of the propellant and how it will behave under different circumstances is a very challenging physics problem. We want to be able to understand how the behaviour of the device might change (and how we could control it) if we switch to more environmentally friendly propellants.
- Why are metered dose inhaler propellants such bad greenhouse gases and why do we need to replace them?
Metered dose inhalers mostly use R-134a (tetrafluoroethane) as their propellant. 1 kg of R-134a is equivalent to 1,430 kg of CO2 when released into the atmosphere. It is a very effective greenhouse gas. For this reason, R-134a is being phased down from use in fridges, air conditioners or household aerosol cans – other fluids like butane, propane, cyclopentane, etc. can be used for such purposes. However, most of these are flammable. We can’t just swap R-134a for one of these in a metered-dose inhaler because the entire operating principle of the device depends upon the propellant’s chemical and physical properties. Changing the propellant requires wholesale redesign of the inhaler, and this is a major engineering challenge because we don’t yet have the tools at our disposal to predict how making such changes will affect the spray. Our research aims to solve this problem.
- Why not just switch to a dry powder inhaler?
For some drugs, we certainly will, but the short answer is that not all propellant driven inhalers can be swapped for dry powder inhalers (DPI) despite some recent reporting that suggests that this should be the solution. There are a few reasons why we can’t just switch all inhalers to dry powder:- Not all drugs are chemically suited for DPIs.
- DPIs cannot be used by young children, the elderly, and those with severe respiratory issues.
- DPIs are more expensive, and thus unsuitable for developing markets, as well as in the USA where over the counter prices are high. Cost is a major factor in people not using their inhaler. Forcing patients onto a more expensive product will lead to a reduction in compliance and more health complications.
- Surely the greenhouse emissions from inhalers are small compared to our total greenhouse emissions. It won’t make much difference. Why bother?
The emissions from inhalers are indeed small relative to emissions from power generation, transport, agriculture, and other sectors – they are thousands of times smaller in terms of CO2-equivalent. However, this does not mean that the problem can simply be ignored. There are several reasons why:- Hydrofluorocarbons are being phased down due to the impact their use is having in developing nations. The production of R-134a will decrease, its cost will rise, and an alternative must be found. The pharmaceutical industry only consumes a few percent of the world supply of R-134a and cannot sustain the market on its own.
- In one year, a typical asthma sufferer will generate an equivalent amount of greenhouse gas from their inhaler use as taking a New York to London plane flight. Given that consumers are now very conscious of their carbon footprint, there is a strong market demand for an inhaler which will give environmentally conscious consumers peace of mind.
- Eliminating emissions from inhalers is relatively cheap and easy compared to the cost and difficulty of transitioning our energy and transport infrastructure. Phase-out of HFCs is one relatively easy step to take when addressing greenhouse gas reduction targets. Australia is leading the way in HFC phase down targets for this reason.
- Redesigning the inhaler provides an opportunity for us to improve the design and function of a product that hasn’t changed much in 50 years. New inhaler designs with new chemistry offer the opportunity to develop custom multi-drug treatments, improved reliability under different temperature and humidity conditions, higher delivery efficiency (since most of the drug never makes it into the lungs in a typical inhaler spray), better shelf life, and many other benefits.
- It’s the right thing to do. Every ton of greenhouse gas not emitted makes a difference to our future, no matter how small. It’s a bit like compound interest – a small change today can add up to a big change in a few decades.
- If HFCs are so bad for the environment, why are we only worrying about this just now?
Actually, scientists have been working with the pharmaceutical industry for years on this problem, however it has received almost no media attention until late 2019. We’ve known about the impact of HFCs on the environment for decades, so why do we persist with them? HFCs were brought in as a replacement for CFCs (chlorofluorocarbons), which you may recall were banned under the Montreal Protocol due to their severe ozone-depleting potential. We have HFCs to thank for the fact that the hole in the ozone layer has not gotten much worse over the last few decades. So, we replaced something that was really bad for the environment (CFCs) with something that was a bit less bad (HFCs). At the time, HFCs were really the only option that provided an immediate drop-in replacement for CFCs, and it worked – we eliminated the use of CFCs in a very short time. We’ve been scaling down the use of HFCs for years, and have already completely eliminated their use in certain products. The Montreal protocol has been amended to mandate the phase down of HFCs like R-134a over a 17 year window. Pharmaceutical inhalers will be one of the last remaining users of R-134a because replacing them is slow and difficult (see question 1). We faced the same challenge eliminating CFCs from inhalers; there is no reason why we can’t do the same thing this time. This time, the underlying physics are more difficult, but the scientific tools we have at our disposal are much more powerful.
- How much will the transition to environmentally friendly propellants cost?
An IPCC 2005 report stated that no major technological breakthroughs were expected in inhaler science, and on this basis the transition would be US $ 1.7b to switch all products to dry powder inhalers. Our research will hopefully provide the breakthrough that will greatly reduce the mitigation cost, because the inhaler itself will not require radically different manufacturing methods, and because we won’t need to rely on more costly dry powder inhalers for every possible product (see question 3).
- Won’t the development of new inhaler technologies just benefit the pharmaceutical industry?
It is true that the development of new inhaler devices will lead to new patents, and that licensing for these patents will benefit those companies which make the significant investment required to develop these new devices. However, this will not significantly disadvantage patients, for the following reasons:- Our work is taxpayer funded (through the Australian Research Council) and as such all results must be released publicly. This means that the findings of our work will not be hidden away, but will be available to everyone.
- The end goal of the research is a product available to consumers at equivalent cost to current inhalers, as price is a major driver of correct use (see question 3).
- The alternative to not doing this is that we have to move wholesale to dry powder inhalers, which are not suitable for all applications and are usually more complex and expensive. This is not viable for developing countries.
- Is using an inhaler really as bad as eating red meat?
Reporting from a Cambridge study by the BBC suggested that this was the case, however that reporting was somewhat misleading. It suggested that patients were to blame for the emissions caused by their inhalers. The authors of that study never said this; they were simply calculating the environmental impact on the NHS in order to convince the government to act. While eating red meat is a choice, using an inhaler is not. Patients should not feel guilty about using their inhaler. Responsibility lies with the pharma industry and government regulators to solve this problem. We are working closely with them to address this issue.

You must be logged in to post a comment.